
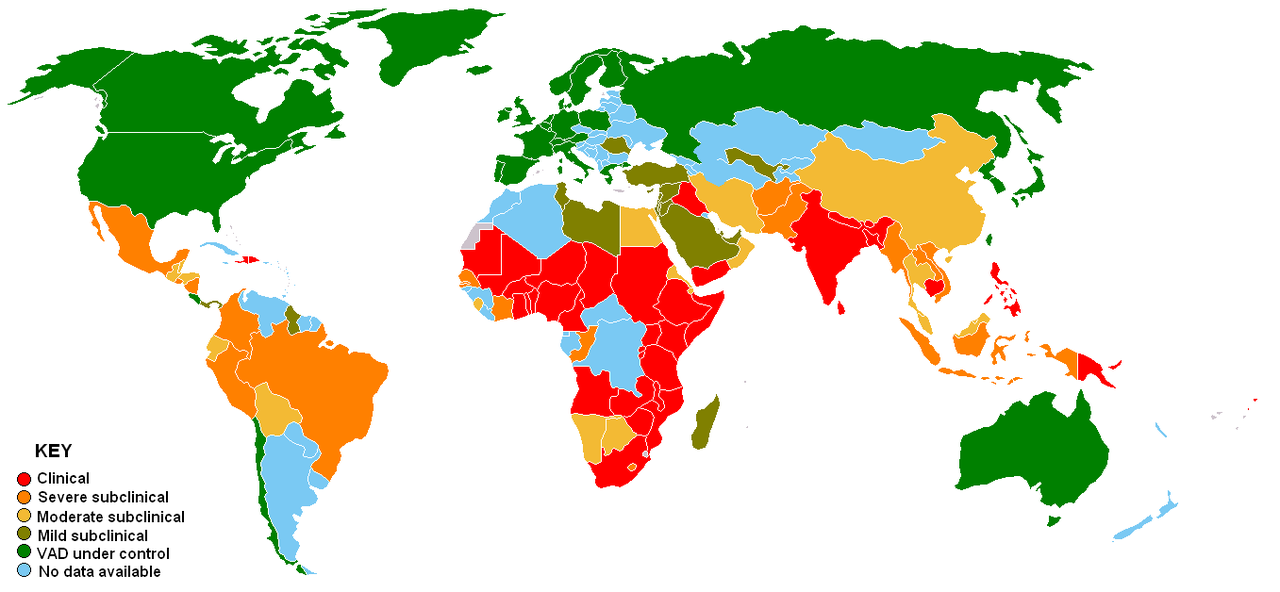
World Distribution of Vitamin A Deficiency

Vitamin A (retinol) is required for the formation of rhodopsin, a photoreceptor pigment in the retina. Vitamin A helps maintain epithelial tissues. Normally, the liver stores 80 to 90% of the body's vitamin A. To use vitamin A, the body releases it into the circulation bound to prealbumin (transthyretin) and retinol-binding protein. β-Carotene and other provitamin carotenoids, contained in green leafy and yellow vegetables and deep- or bright-colored fruits, are converted to vitamin A. Carotenoids are absorbed better from vegetables when they are cooked or homogenized and served with some fats or oils.
Retinol activity equivalents (RAE) were developed because provitamin A carotenoids have less vitamin A activity than preformed vitamin A; 1 µg retinol = 3.33 IU.
Synthetic vitamin analogs (retinoids) are being used increasingly in dermatology. The possible protective role of β-carotene, retinol, and retinoids against some epithelial cancers is under study. However, risk of certain cancers may be increased after β-carotene supplementation.
Retinol activity equivalents (RAE) were developed because provitamin A carotenoids have less vitamin A activity than preformed vitamin A; 1 µg retinol = 3.33 IU.
Synthetic vitamin analogs (retinoids) are being used increasingly in dermatology. The possible protective role of β-carotene, retinol, and retinoids against some epithelial cancers is under study. However, risk of certain cancers may be increased after β-carotene supplementation.
VITAMIN A DEFICIENCY

Vitamin A deficiency can result from inadequate intake, fat malabsorption, or liver disorders. Deficiency impairs immunity and hematopoiesis and causes rashes and typical ocular effects (eg, xerophthalmia, night blindness). Diagnosis is based on typical ocular findings and low vitamin A levels. Treatment consists of vitamin A given orally or, if symptoms are severe or malabsorption is the cause, parenterally.
Vitamin A deficiency occurs with protein-energy malnutrition (marasmus or kwashiorkor) for the reason that of dietary deficiency (but vitamin A storage and transport will also be impaired). This happens there are problems in converting carotene to vitamin A, or reduced absorption, storage, or transport of vitamin A. This happens in coeliac disease, tropical sprue, giardiasis, cystic fibrosis, other pancreatic disease, cirrhosis, duodenal bypass surgery, and bile duct obstruction.
Bone and teeth development and regeneration.
Vitamin A plays an indispensable aspect in the strengthening of bones and the development of the skeletal structure in humans, right from birth to old age. Absence of vitamin A can lead to weaker bones, making them brittle and excess of a typical same can create the bone vulnerable to dangerous diseases like cancer, osteoporosis while others. Vitamin A is likewise designed to prevent tooth and gum problems.
Vision and sight improvement
Vitamin A compound retinol made use of from the eye retina under the reception of sunshine and transfer of images to the brain. Sufficient quantities of Vitamin A are involved to ensure clearer visibility and sharper eyesight. Deficiency could cause night blindness and other eye disorders similar to cataracts, etc.
Smooth disease-free skin
Vitamin A is beneficial for coping with the several skin problems like acne, pimples, sunburns, pigmentation, etc. This holds true both for the external skin surface as well as the lining of many internal organs. Vitamin A’s function in cell formation and regeneration enables person to maintain the skin free of any ailments. Healing of wounds, deficiency of wrinkles, removal of acne, all is by way of the credit rating of Vitamin A.
Reproduction
The presence of sufficient Vitamin A is crucial for the sperm growth. It helps equip smooth pregnancy, trouble free menstrual cycles, etc. Vitamin A is also utilized by women who are pregnant to address the danger of transmitting HIV for their unborn child.
Strengthening immunity
Vitamin A is required of the daily functioning of many immune system. It plays a central aspect in causing the white blood cells, that applied in fighting infections thus preventing diseases and illnesses. Red blood cell formation is also increased due to Vitamin A in the body.
Cell development, formation, regeneration
Every second, every minute, hundreds and many thousands of cells are destroyed and created in the body. Vitamin A consists of a major role to act like under the development of new cells, repair of injured or sick cells.
Etiology
Primary vitamin A deficiency is usually caused by prolonged dietary deprivation. It is endemic in areas such as southern and eastern Asia, where rice, devoid of β-carotene, is the staple food. Xerophthalmia due to primary deficiency is a common cause of blindness among young children in developing countries.
Secondary vitamin A deficiency may be due to decreased bioavailability of provitamin A carotenoids or to interference with absorption, storage, or transport of vitamin A. Interference with absorption or storage is likely in celiac disease, cystic fibrosis, pancreatic insufficiency, duodenal bypass, chronic diarrhea, bile duct obstruction, giardiasis, and cirrhosis. Vitamin A deficiency is common in prolonged protein-energy undernutrition not only because the diet is deficient but also because vitamin A storage and transport is defective. In children with complicated measles, vitamin A can shorten the duration of the disorder and reduce the severity of symptoms and risk of death.
Every second, every minute, hundreds and many thousands of cells are destroyed and created in the body. Vitamin A consists of a major role to act like under the development of new cells, repair of injured or sick cells.
Etiology
Primary vitamin A deficiency is usually caused by prolonged dietary deprivation. It is endemic in areas such as southern and eastern Asia, where rice, devoid of β-carotene, is the staple food. Xerophthalmia due to primary deficiency is a common cause of blindness among young children in developing countries.
Secondary vitamin A deficiency may be due to decreased bioavailability of provitamin A carotenoids or to interference with absorption, storage, or transport of vitamin A. Interference with absorption or storage is likely in celiac disease, cystic fibrosis, pancreatic insufficiency, duodenal bypass, chronic diarrhea, bile duct obstruction, giardiasis, and cirrhosis. Vitamin A deficiency is common in prolonged protein-energy undernutrition not only because the diet is deficient but also because vitamin A storage and transport is defective. In children with complicated measles, vitamin A can shorten the duration of the disorder and reduce the severity of symptoms and risk of death.
Symptoms and Signs - Impaired dark adaptation of the eyes, which can lead to night blindness, is an early symptom.
Xerophthalmia

Keratoconjunctivitis sicca (KCS) - also called keratitis sicca, xerophthalmia or dry eye syndrome (DES) is an eye disease caused by eye dryness, which, in turn, is caused by either decreased tear production or increased tear film evaporation
Xerophthalmia
Keratoconjunctivitis sicca (KCS) - also called keratitis sicca, xerophthalmia or dry eye syndrome (DES) is an eye disease caused by eye dryness, which, in turn, is caused by either decreased tear production or increased tear film evaporation
Keratinization of the skin and of the mucous membranes in the respiratory, GI, and urinary tracts can occur. Drying, scaling, and follicular thickening of the skin and respiratory infections can result. Immunity is generally impaired.
The younger the patient, the more severe are the effects of vitamin A deficiency. Growth retardation and infections are common among children. Mortality rate can exceed 50% in children with severe vitamin A deficiency.
Diagnosis - Serum retinol levels, clinical evaluation, and response to vitamin A.
Ocular findings suggest the diagnosis. Dark adaptation can be impaired in other disorders (eg, zinc deficiency, retinitis pigmentosa, severe refractive errors, cataracts, diabetic retinopathy). If dark adaptation is impaired, rod scotometry and electroretinography are done to determine whether vitamin A deficiency is the cause.
Serum levels of retinol are measured. Normal range is 28 to 86 μg/dL (1 to 3 µmol/L). However, levels decrease only after the deficiency is advanced because the liver contains large stores of vitamin A. Also, decreased levels may result from acute infection, which causes retinol-binding protein and transthyretin (also called prealbumin) levels to decrease transiently. A therapeutic trial of vitamin A may help confirm the diagnosis.
Ocular findings suggest the diagnosis. Dark adaptation can be impaired in other disorders (eg, zinc deficiency, retinitis pigmentosa, severe refractive errors, cataracts, diabetic retinopathy). If dark adaptation is impaired, rod scotometry and electroretinography are done to determine whether vitamin A deficiency is the cause.
Serum levels of retinol are measured. Normal range is 28 to 86 μg/dL (1 to 3 µmol/L). However, levels decrease only after the deficiency is advanced because the liver contains large stores of vitamin A. Also, decreased levels may result from acute infection, which causes retinol-binding protein and transthyretin (also called prealbumin) levels to decrease transiently. A therapeutic trial of vitamin A may help confirm the diagnosis.
Prevention
The diet should include dark green leafy vegetables, deep- or bright-colored fruits (eg, papayas, oranges), carrots, and yellow vegetables (eg, squash, pumpkin). Vitamin A–fortified milk and cereals, liver, egg yolks, and fish liver oils are helpful. Carotenoids are absorbed better when consumed with some dietary fat. If milk allergy is suspected in infants, they should be given adequate vitamin A in formula feedings.
In developing countries, prophylactic supplements of vitamin A palmitate in oil 60,000 RAE (200,000 IU) po every 6 mo are advised for all children between 1 and 5 yr of age; infants < 6 mo can be given a one-time dose of 15,000 RAE (50,000 IU), and those aged 6 to 12 mo can be given a one-time dose of 30,000 RAE (100,000 IU).
Treatment
Vitamin A palmitate
Dietary deficiency is traditionally treated with vitamin A palmitate in oil 60,000 IU po once/day for 2 days, followed by 4500 IU po once/day. If vomiting or malabsorption is present or xerophthalmia is probable, a dose of 50,000 IU for infants < 6 mo, 100,000 IU for infants 6 to 12 mo, or 200,000 IU for children > 12 mo and adults should be given for 2 days, with a third dose at least 2 wk later. The same doses are recommended for infants and children with complicated measles. Infants born of HIV-positive mothers should receive 50,000 IU (15,000 RAE) within 48 h of birth. Prolonged daily administration of large doses, especially to infants, must be avoided because toxicity may result.
For pregnant or breastfeeding women, prophylactic or therapeutic doses should not exceed 10,000 IU (3000 RAE)/day to avoid possible damage to the fetus or infant.
Key Points
Vitamin A deficiency usually results from dietary deficiency, as occurs in areas where rice, devoid of β-carotene, is the staple food, but it may result from disorders that interfere with the absorption, storage, or transport of vitamin A.
Ocular findings include impaired night vision (early), conjunctival deposits, and keratomalacia.
In children with severe deficiency, growth is slowed and risk of infection is increased.
Diagnose based on ocular findings and serum retinol levels. Treat with vitamin A palmitate.
Vitamin A deficiency usually results from dietary deficiency, as occurs in areas where rice, devoid of β-carotene, is the staple food, but it may result from disorders that interfere with the absorption, storage, or transport of vitamin A.
Ocular findings include impaired night vision (early), conjunctival deposits, and keratomalacia.
In children with severe deficiency, growth is slowed and risk of infection is increased.
Diagnose based on ocular findings and serum retinol levels. Treat with vitamin A palmitate.
VITAMIN A TOXICITY
Vitamin A toxicity can be acute (usually due to accidental ingestion by children) or chronic. Both types usually cause headache and increased intracranial pressure. Acute toxicity causes nausea and vomiting. Chronic toxicity causes changes in skin, hair, and nails; abnormal liver test results; and, in a fetus, birth defects. Diagnosis is usually clinical. Unless birth defects are present, adjusting the dose almost always leads to complete recovery.
Acute vitamin A toxicity in children may result from taking large doses (> 300,000 IU [> 100,000 RAE]), usually accidentally. In adults, acute toxicity has occurred when arctic explorers ingested polar bear or seal livers, which contain several million units of vitamin A.
Chronic toxicity in older children and adults usually develops after doses of > 30,000 RAE (> 100,000 IU)/day have been taken for months. Megavitamin therapy is a possible cause, as are massive daily doses (50,000 to 120,000 RAE [150,000 to 350,000 IU]) of vitamin A or its metabolites, which are sometimes given for nodular acne or other skin disorders. Adults who consume > 1500 RAE (> 4500 IU)/day of vitamin A may develop osteoporosis. Infants who are given excessive doses (6,000 to 20,000 RAE [18,000 to 60,000 IU]/day) of water-miscible vitamin A may develop toxicity within a few weeks. Birth defects occur in children of women receiving isotretinoin (which is related to vitamin A) for acne treatment during pregnancy.
Although carotene is converted to vitamin A in the body, excessive ingestion of carotene causes carotenemia, not vitamin A toxicity. Carotenemia is usually asymptomatic but may lead to carotenosis, in which the skin becomes yellow. When taken as a supplement, β-carotene has been associated with increased cancer risk; risk does not seem to increase when carotenoids are consumed in fruits and vegetables.
Symptoms and Signs
Although symptoms may vary, headache and rash usually develop during acute or chronic toxicity. Acute toxicity causes increased intracranial pressure. Drowsiness, irritability, abdominal pain, nausea, and vomiting are common. Sometimes the skin subsequently peels.
Early symptoms of chronic toxicity are sparsely distributed, coarse hair; alopecia of the eyebrows; dry, rough skin; dry eyes; and cracked lips. Later, severe headache, pseudotumor cerebri, and generalized weakness develop. Cortical hyperostosis of bone and arthralgia may occur, especially in children. Fractures may occur easily, especially in the elderly. In children, toxicity can cause pruritus, anorexia, and failure to thrive. Hepatomegaly and splenomegaly may occur.
In carotenosis, the skin (but not the sclera) becomes deep yellow, especially on the palms and soles.
Diagnosis
Clinical evaluation
Diagnosis is clinical. Blood vitamin levels correlate poorly with toxicity. However, if clinical diagnosis is equivocal, laboratory testing may help. In vitamin A toxicity, fasting serum retinol levels may increase from normal (28 to 86 μg/dL [1 to 3 µmol/L]) to > 100 μg/dL (> 3.49 µmol/L), sometimes to > 2000 μg/dL (> 69.8 µmol/L). Hypercalcemia is common.
Differentiating vitamin A toxicity from other disorders may be difficult. Carotenosis may also occur in severe hypothyroidism and anorexia nervosa, possibly because carotene is converted to vitamin A more slowly.
Prognosis
Complete recovery usually occurs if vitamin A ingestion stops. Symptoms and signs of chronic toxicity usually disappear within 1 to 4 wk. However, birth defects in the fetus of a mother who has taken megadoses of vitamin A are not reversible. recommended treatment is to stop Vitamin A administeration.
Key Points
Vitamin A toxicity can be caused by ingesting high doses of vitamin A—acutely (usually accidentally by children) or chronically (eg, as megavitamin therapy or treatment for skin disorders).
Acute toxicity causes rash, abdominal pain, increased intracranial pressure, and vomiting.
Chronic toxicity causes rash, increased intracranial pressure, sparse and coarse hair, dry and rough skin, and arthralgia; risk of fractures is increased, especially in the elderly.
Diagnose based on clinical findings.
When vitamin A is stopped, symptoms (except birth defects) usually resolve within 1 to 4 wk.
Sources: www.merckmanuals.com
Differentiating vitamin A toxicity from other disorders may be difficult. Carotenosis may also occur in severe hypothyroidism and anorexia nervosa, possibly because carotene is converted to vitamin A more slowly.
Prognosis
Complete recovery usually occurs if vitamin A ingestion stops. Symptoms and signs of chronic toxicity usually disappear within 1 to 4 wk. However, birth defects in the fetus of a mother who has taken megadoses of vitamin A are not reversible. recommended treatment is to stop Vitamin A administeration.
Key Points
Vitamin A toxicity can be caused by ingesting high doses of vitamin A—acutely (usually accidentally by children) or chronically (eg, as megavitamin therapy or treatment for skin disorders).
Acute toxicity causes rash, abdominal pain, increased intracranial pressure, and vomiting.
Chronic toxicity causes rash, increased intracranial pressure, sparse and coarse hair, dry and rough skin, and arthralgia; risk of fractures is increased, especially in the elderly.
Diagnose based on clinical findings.
When vitamin A is stopped, symptoms (except birth defects) usually resolve within 1 to 4 wk.
Sources: www.merckmanuals.com
www.sanjeevan.in
waytoenliven.com
www.nutraingredients.com
No comments:
Post a Comment